Liberals’ “Alternative Facts” on Capping Entitlement Spending
Here’s a policy riddle for you: When is a spending cap not a spending cap? The answer: When a liberal finds it politically inconvenient.
During the confirmation hearing for Health and Human Services Secretary-designee Alex Azar, a staffer for the liberal Center for Budget and Policy Priorities tweeted that Azar supported capping Medicaid. I noted that meant he supported capping Medicaid spending like the caps Democrats enacted as part of Obamacare—and that’s when the fun began.
Then I pointed out that Section 3403 of Obamacare charges the Independent Payment Advisory Board (IPAB) with enforcing a cap on per-beneficiary spending in Medicare. She responded by saying that IPAB contains restrictions on “rationing health care, raising Medicare’s premiums or cost sharing, cutting benefits, or restricting eligibility.”
That response, while accurate, misses the point. First of all, while the law prohibits Medicare from “rationing” benefits, neither Obamacare nor any other law “defines” rationing. Former Health and Human Services secretary Kathleen Sebelius testified to Congress in 2011 that HHS would need to undertake rulemaking to define “rationing.” However, as I noted this summer, “the Obama Administration never even proposed rules ‘protecting’ Medicare beneficiaries from rationing under the IPAB per capita caps—so how meaningful can those protections actually be?”
Capping Spending Does Indeed Reduce It
Second, a cap on spending, by definition, will reduce spending. The implication that one form of cap on spending in Medicare will have no ramifications whatsoever for beneficiaries, while another form of cap on spending in Medicaid will lead to proverbial death and destruction, strains credulity.
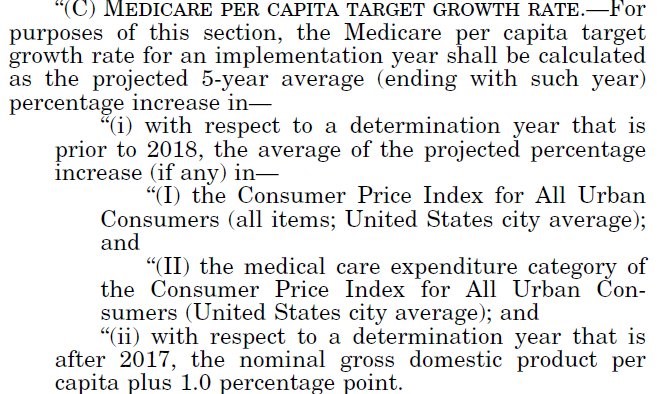
But putting those distinctions aside for a second, I asked whether Obamacare capped Medicare spending. I sent links to the portions of Section 3403 that 1) establish a target growth rate for Medicare and 2) instruct IPAB to develop recommendations to reduce spending to meet that target—the definition of a cap in my book, and probably anyone else’s as well.
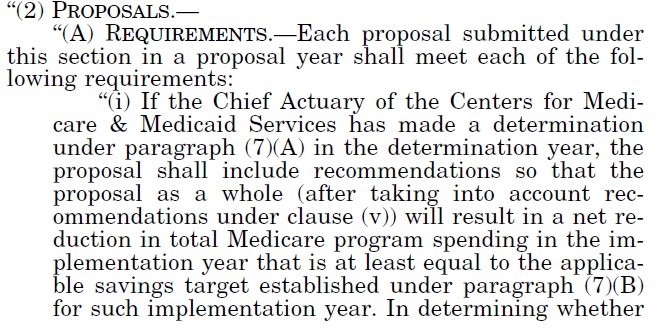
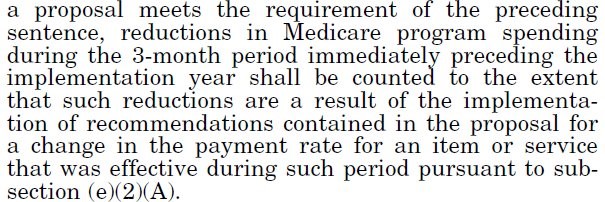
I asked a simple yes-no question: While they might be implemented in different ways than the caps in Republicans’ “repeal-and-replace” bills, doesn’t IPAB limit the growth rate of Medicare spending to meet a cap?
Answer came there none.
Politically Inconvenient Truths
The political hack—erm, I mean, “analyst”—in question, from the Center for Budget and Policy Priorities, has more than enough health policy experience to recognize a spending cap. According to the center’s website, she served in senior roles in California’s Medicaid program, worked as the primary health staffer for former U.S. senator Al Franken (D-MN), and holds a master’s degree in health policy. She knows better—she just chose not to.
As I have written previously, Democrats don’t want to admit that they imposed per capita spending caps in Medicare as part of Obamacare. They may still fear the political consequences of capping Medicare spending—and more importantly, do not want to give Republicans political “cover” to impose similar caps in Medicaid.
So rather than admit the obvious—yes, Democrats did impose spending caps in Medicare (albeit in a slightly different form than Republicans’ Medicaid proposals last year) as part of Obamacare—this person chose to obfuscate, deflect, deny, and ultimately join Twitter’s version of the Witness Protection Program rather than admit the politically inconvenient truth. And beclowned herself in the process.
After the “repeal-and-replace” process of 2017, I know full well what it means to tell politically inconvenient truths. Going out on a limb to point out flaws in alternatives to Obamacare won me no small amount of flack from others on the Right, and may have cost me business to boot.
But at bottom, I consider myself a conservative health policy analyst, not a Republican one. As such, I feel an obligation to call “balls-and-strikes” based solely on policy, regardless of party. Doing otherwise would harm my reputation and integrity. And in policy circles in this town, one’s good name is the only thing you’ve got.
People can propose “alternative facts” all they like, but not without cost. After our Twitter tete-a-tete, I think less of the analyst in question, and of the Center for Budget and Policy Priorities for employing her. While liberals can talk all they like about a “wonk gap,” or about Republican “science deniers,” they appear to have some in their own midst as well. Just ask liberal health analysts about IPAB’s per capita caps.
This post was originally published at The Federalist.